















Through the years we have these feathers in our cap.
Centre for Operations Research and Training (CORT) is a multi-disciplinary social science research and training organization, specializing in population, health including reproductive health and family planning, water, sanitation and hygiene, youth, gender equity, education, labour force, living wage, other social development issues and capacity building. Established in early 1991, by a group of committed social scientists, CORT is recognized as a leading research, training and consultancy organization in the country. CORT is registered with Udyog Aadhaar registration under Ministry of Micro Small & Medium Enterprises (MSME).
CORT aspires to contribute meaningfully in national development and evidence based policy decision making by undertaking policy relevant research on issues that are impeding the performance of the health and social sectors and build capacity of human resources through trainings.

CORT undertakes quantitative and qualitative research to understand factors influencing performance of health and other social sectors, to assess/test alternative strategies and interventions to improve functioning of the programs. Overall, CORT plays a catalyst role in national development and contributes its expertise towards-
A) Undertaking policy relevant research on issues of national importance with special emphasis to reproductive health, adolescent, gender, equity and disadvantaged groups,
B) Lead monitoring and evaluation (M&E) of large national programs and participate as M&E partner in important implementation programs,
C) Build capacity of NGOs, research institutions, program managers, service providers and other organizations to improve performance of programs,
D) Increase utilization of research through advocacy, dissemination and networking.
These strategic thrust areas are ethically addressed and analyzed with the lens of gender equity.
• Access choice and quality of RH and FW services
• Safe motherhood and child survival
• Water and Sanitation
• Education: access, quality and dropout
• Gender equity and violence
• Nutrition: causes and consequences
• Abortion and post abortion care
• Living Wages
• Access, quality and utilization of health services
• Adolescent’s RH, education and empowerment
• Child labour, employment and poverty
• STI, HIV and AIDS
• Capacity Building
• Community Mobilization
• Rural Development
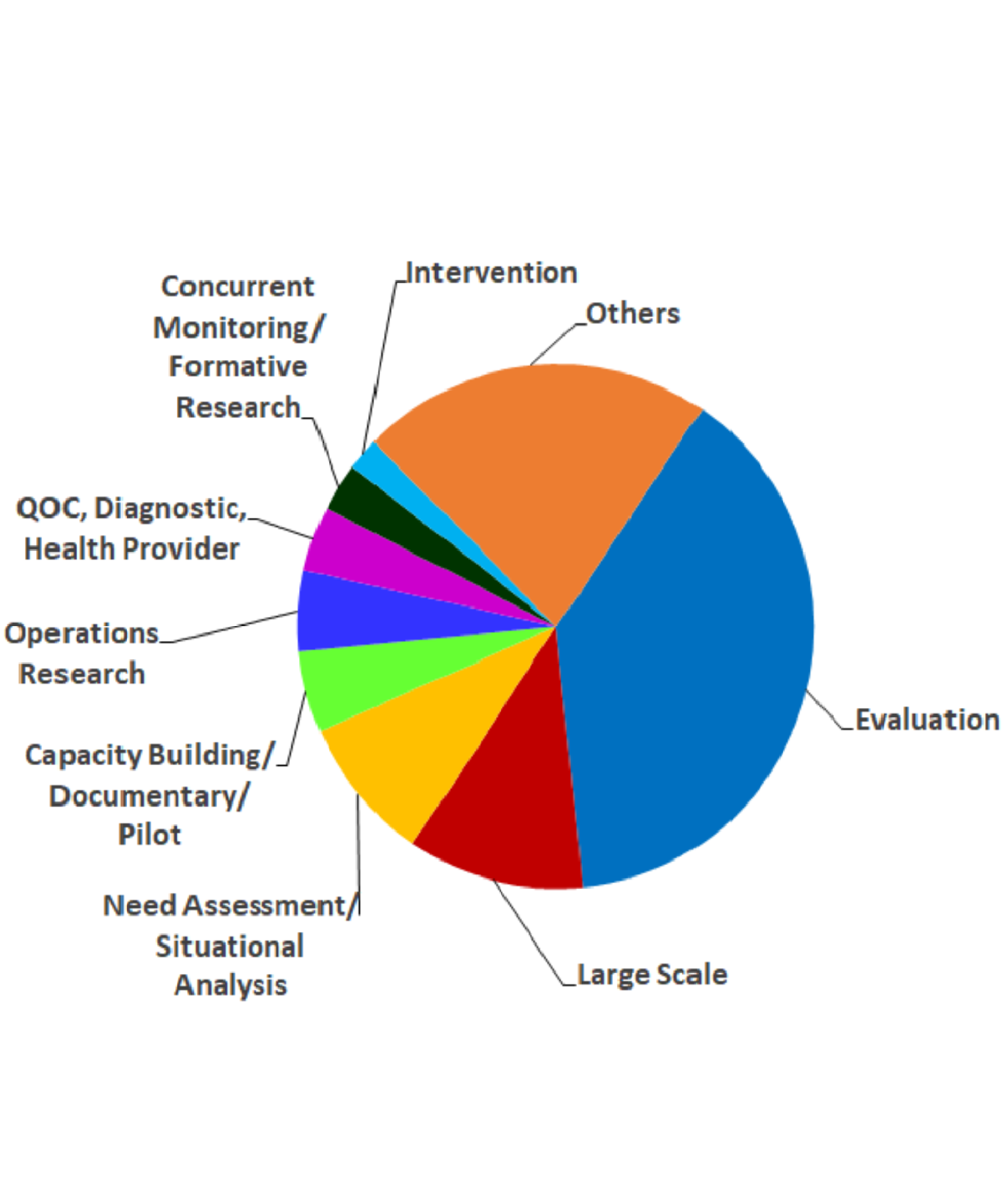
Most studies use both quantitative and qualitative methods to present a comprehensive scenario. Nature of studies implemented has been diverse including operations research, formative studies, need assessment, concurrent monitoring, situational analysis, baseline–end line surveys, pilot studies and serving as monitoring and evaluation partner. CORT has also been doing capacity building and process documentation. Sample size covered in these varied widely, from less than 1000 to more than 50000 households.
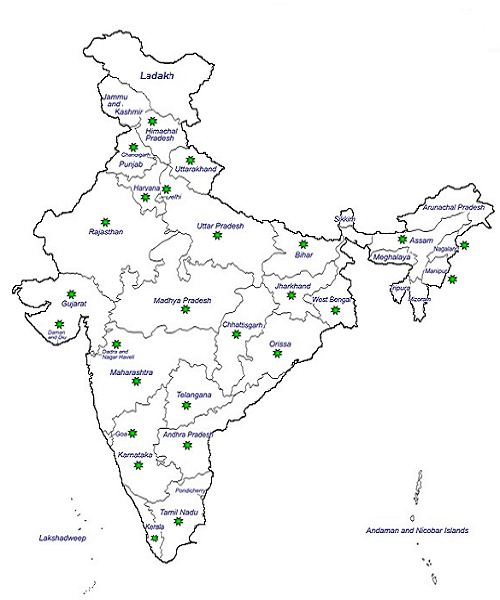
CORT has covered almost all the states and union territories of India while implementing its various studies. It preferably utilizes local human resources in carrying out the activities effectively and continues to maintain its team members' network across all the states and union territories worked.
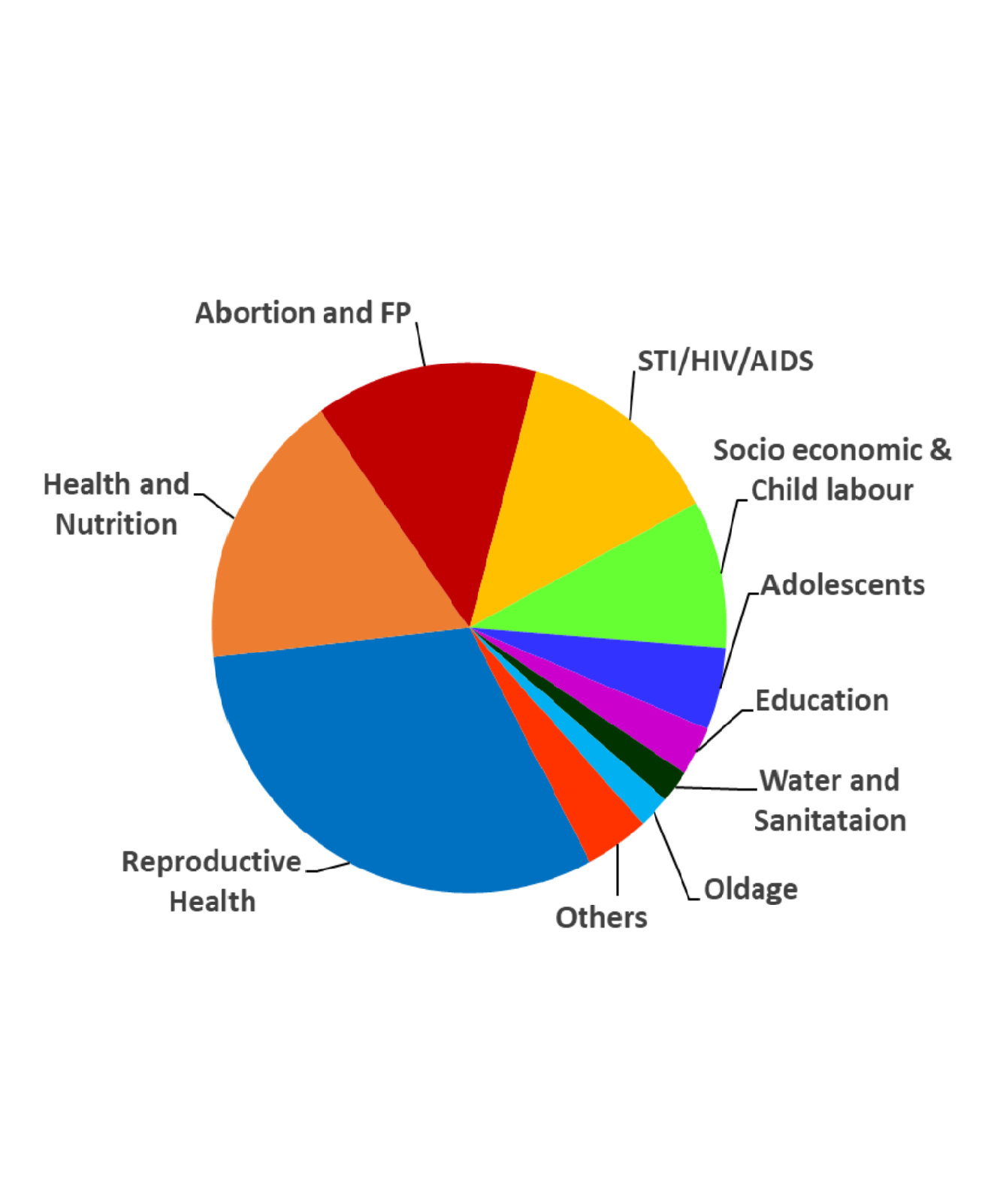
CORT’s initiative has been enriching and challenging as it has worked across a wide spectrum of developmental sectors. Our studies have traversed across various issues ranging from health, family planning, abortion, nutrition, sexual and gender based violence, social and economical issues, gender equity, child labour, livelihood, education, water and sanitation, solid waste management, health facilities at various levels with different perspectives, etc.
CORT has latest technology peripherals and software to manage huge data processing in house. There is an entire unit for data processing which includes data entry, scrutiny, editing, analysis and application of advanced statistics.

The well equipped computer unit facilitates data management and processing trainings of university students, NGOs, professional and research personnel. CORT offers technical support in data processing including data entry, scrutiny, editing and analysis with application of statistics, to various institutions as per their requirement.

The data centre is utilized for data processing including data entry, editing, scrutiny and analysis. Computer Assisted Personal Interviewing (CAPI) technique is used in data collection. Data management software is developed in-house for various CORT activities such as monitoring, quality control and user friendly data entry, editing & MIS packages.

Study reports, presentations, IEC materials, dissemination material, etc., are all well designed and laid out tailor made to make them attractive and easy to read as per the target audiences. All the related activities including, formatting, layout, designing, scaning and editing imaging, etc. are done by in-house experts.
CORT provides services to a wide range of international and national client institutions in its areas of core competence. Selected client institutions includes:


High quality contraceptive counselling and method provision are fundamental to a human rights based approach to family welfare services. High quality counselling entails providing individuals with personalized information about available methods and unbiased decision support to select the method that will best suit their needs.
A formative study was taken up to facilitate development of a measurement scale that would gauge women’s perceptions of quality of contraceptive counselling. Eight focus group discussions were conducted with contraceptive users in both urban and rural areas to develop survey tool designed to be used in future research to measure quantitatively women’s perceptions of the quality of the interaction with health care providers of contraception.
Focus was on clients’ experiences with contraceptive counselling from health providers, their perspectives on what constitutes good interactions with providers and feedback on potential scale items. During FGDs, women were asked about specific elements of their interaction with the providers including how they perceive privacy, confidentiality, respect, trust and empathy.
Participants were overall grateful for the advice and support they received from providers, though many wanted more information about options for sterilization and reversible contraception. A common theme was desire for more proactive information about side effects of their chosen method and how to manage them. Women expressed the final decision about contraceptive use should be up to the woman, though some reported experiences of some sort of pressure from providers to use an intrauterine device (IUD), particularly postpartum. In a few cases, participants described providers inserting IUDs without their permission.

Research in high income countries has demonstrated that antenatal care delivered in a group may be an effective way to improve the provision, experiences, and outcomes of care for pregnant woman and new born.
A feasibility study was undertaken to test it in low, middle income countries. A “generic” model was tailored for local levels and used in urban setting in Gujarat, India. Four demonstrations of a session of the model was done with administrators, physicians, ANMs, pregnant women, and support persons from public and private health facilities in Gujarat, India. In all, 5 physicians, 7 ANMs and one anganwadi worker participated in the demonstration for care providers. For care receivers, 38 individuals: 29 pregnant women and nine support persons (3 mothers, one mother-in-law, and 5 husbands) participated in three group demonstrations. Each participant took part either in in-depth interviews, survey or focus group discussions.
Demonstration revealed its acceptability among respondents who were happy and expressed support and enthusiasm for the model. A women side “That (group ANC) was good, privacy was good, and the way she told me to get up, from supine to side line and side line to supine that was also very good. Eye contact maintained was important”. A provider appreciating self-assessment of blood pressure and weight said “It was a very novel idea. If the woman does her own assessment she gets the feelings of ownership...” Participants also liked the session on nutrition, learnt new things by sharing their concerns and learning from each other’s experience. Husbands also appreciated learning about nutrition and about discomfort and danger signs during pregnancy from the doctor. In one FGD, women did share their concern regarding time being too long for group ANC.
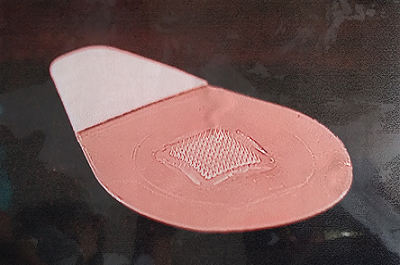
Modern contraceptive prevalence in India is 48% with most women using permanent contraception. Need of increasing long-term temporary methods and choice continues to be a challenge. As part to increase contraceptive choice and user-friendly method efforts are being made to test acceptability of contraceptive microarray patch (MAP). This could expand the range of self-administrable methods.
FHI 360 planned a Discreet Choice Experiment (DCE) survey in New Delhi, India that was conducted by CORT. Women were requested to assess preferences for potential product attributes: effect on menstruation, duration of effectiveness, location, rash after application, and patch size.
For the study, three Municipal Corporations and two zones of Delhi were selected randomly. Zone Lists of Census Enumeration Blocks (CEBs) were used to select 10 CEBs (5 urban and 5 rural/peri urban areas) using systematic sampling method. Mapping listing of all households in selected CEBs gave a list of users and non-users of contraception. Using systematic sampling method, 40 women per CEB were selected (excluding users of permanent contraceptive method). Ten cognitive interviews were conducted with purposively selected informants to assess their understanding if attributes, pictures, font and presentation of the DCE survey appropriately conveyed the message to women.
In all, 496 respondents were presented 10 sets of two choice pairs of MAP designs on tablets. Choice pairs were randomly generated to have balanced overlap between attribute levels. Women preferred a regular period over an irregular or no period, and a six-month duration to three or one month. We found that women were excited about this method, but they would prefer a product that would offer several months of pregnancy protection and not have menstrual side effects.

Period during and immediately after the child birth always remains critical for maternal and new-born survival and well being. A holistic approach of “Care Around Birth” (CAB) integrates technical interventions in the health system, strengthening, quality improvement techniques and respectful maternity care practices to optimize QOC at and around birth.
The study made an attempt to assess modalities related to CAB approach such as knowledge and current practices in maternal and new born care in labour room environment and management of complications.
A mixed method approach using qualitative and quantitative technique was used. Study covered 26 L2 and 25 L3 facilities located in 6 states. Labour room practices, and knowledge assessment of health care providers were done. Interviews with medical officers, district and state officials were conducted. 408 beneficiary woman visiting for delivery were observed till two hours of post- delivery.
Positive changes in readiness of labour room were visible in basic amenities and support services from baseline. Documentation and recording practices had improved. Overall competency scores in knowledge among health providers improved, which was also corroborated during observation of deliveries such as improved ability to monitor progress of labour, provision of AMTSL, postnatal monitoring and infection prevention. Staff members expressed constrains in areas like maintaining privacy in labor rooms, intra and interdepartmental coordination, low confidence levels among some to handle alone and extended duty hours. Beneficiaries appreciated availability of different amenities. On elements of Respectful Maternity Care, in 99.7% the behaviour of service provider was gentle, comforting and reassuring. Beneficiaries felt the service provider was supportive, encouraging and comforting.

Swachh Bharat Abhiyan, launched on October 2, 2014, aims to make India free from open-defecation and achieve universal sanitation by 2019. The study funded by WaterAids assessed situation of Water and Sanitation Hygiene (WASH) in 9 states of India. The key focus was to understand the process of implementation assessing inputs (manpower, money, material, and time) and outputs (immediate services, improved behaviour change, staff trained, materials distributed), pitfalls and scope for further improvements of the program. Community was asked about their awareness about SBM program, its benefits, knowledge about hygiene, current practices, barriers and facilitating factors in adopting desired behaviour change.
The methodology consisted of desk review, examining the data on current status, cross sectional survey of 162 Gram Panchayats interviewing 3,904 households, 453 schools, 830 teachers and 4,806 students spread over 34 districts and 9 states of India.
The study revealed that students groups, Bal Sansads, Vanar Sena, and Bal Kamando, monitored to keep the village open defecation free (ODF) and ensured that people or students do not defecate in open. Over 95% households had drinking water facility in vicinity, 20% treated water to make it safe, and one-third of the rural households had toilet facility. In 64% of all households, adolescents and 60% households elderly age group (60 years or more) reported open defecation. Majority (67-84%) washed hands before and after eating, and after defecation.
Most schools had toilet facilities and hand washing stations, but only 76% schools had separate toilets for boys and girls. A functional toilet was available per 76 boys and one per 66 girls in schools. Only one in five schools covered, had facility for girls to manage menstrual hygiene that were almost non-existent in Bihar, Chhattisgarh, Odisha and Jharkhand. Students had inculcated the practice of washing hands with soap and water, as observed that 82% students washed their hands after toilet use and 95% before eating. Majority (84%) schools had School Management Committee (SMC) that monitored WASH facilities and ensured that Solid waste was disposed regularly from the school. There is need to further streamline and monitor the aspects of SBM.

Solid Waste Management (SWM) is one of the basic essential services provided by Municipal authorities to keep cities clean. Yet, it remains a poorly rendered service. Reasons identified largely points to the use of a system that is unscientific, outdated, and inefficient with low coverage of population.
The baseline study supported by Infrastructure Leasing & Financial Services Limited (ILFS) attempted to assess perception of people from various aspects related to SWM in Vadodara. It covered various sectors including residential, commercial, institutional as well as spots of tourism visit. The study covered 1,040 individuals across socio-economic, geographic and residential/ non-residential areas and tried to get people’s perspective on the possible improvement opportunities in the SWM services.
Waste was collected every day in residential areas (67 percent) and commercial institutions (95 percent). Both public and private agencies were involved in collecting waste from the premises informing households by blowing whistle. In tourist spots like gardens, heritage buildings, platforms and its entrances etc., most (92%) respondents reported that dustbins for waste collection were located as desired and waste was regularly collected. Tourists suggested for improving timely and regular cleanliness (32%), educating people regarding cleanliness (32%), punishing and imposing penalty on throwing plastic waste (26%), need for prompt and quick disposal of waste and not to burn the waste (5-10%).
Respondents pointed out the need to reach remote areas for garbage collections, stop leachate dripping, have fixed timing of collection and spend adequate time at the place of garbage collection. Collection of door to door solid waste needs to improve particularly during monsoon season when there are higher chances of diseases outbreak. In view of respondents, bad odour, movement of stray dogs, pigs, and cattle’s and rodents calls for an action.

Adolescence in life cycle is a phase of rapid growth and development during which physical, physiological and behavioural changes occur. Centre for Catalyzing Change aims to create an empowering eco-system and positively impact the life of adolescents in Gujarat through development and transaction of a graded Adolescence Education Programme (AEP) curriculum. It covers 6, 7, 8, 9 and 11 classes in middle and secondary government schools in 33 districts of Gujarat. A study of need assessment was conducted in 3 districts of Gujarat in primary and secondary government schools to gain in-depth understanding of the socio-cultural context with respect to sexual and reproductive health and rights of adolescents. The study used mixed-method approach to collect required data from school students by using self-administered questionnaires with the 200 secondary students of class 9 and 11. Assistance was provided to 300 primary students from class 6-8. Key stakeholders including 9 principals, 15 teachers, 10 community members and 6 officials at district and state levels were interviewed to get an overview of the adolescent program and needs. Results show that students, more girls, received books (85%), scholarship (71%), cycles (35%) and school uniforms (11%) as government aid. Only 57% students were aware of legal age for marriage for boys and girls, 15-26% knew about contraception, and had mixed views about gender equality. Students were more aware of physical changes during adolescence, than of internal or emotional ones. The additive index indicates that 40% students had high score and 58% had medium score in dealing with stress. Majority (81%) girls discussed everything with their mothers compared to 66% boys, 72% boys shared their concerns with fathers. Nearly 46-60% (with higher percent of girls) disagreed common beliefs regarding not trusting person with light eyes, dressing sense defining character of girls and black cat crossing road as bad omen. Students felt that disability can be a natural occurrence (55%), but interferes in person’s ability (27%), and also felt that something can be done to help them (41%). Study show that based on scoring, comprehensive knowledge on life skill (52%), health and hygiene (26%), HIV/AIDS (22%), road safety and safe internet use (33% low) among school students was low. Stakeholders felt that due to lack of time, over burden, lack of manpower, this topics could not be dedicated as subject. Few reported resistance in teaching these topics to adolescent.

Out of the 152 countries, India ranked 127th in the list based on the UNDP’s Gender Inequality Index – 2014. The index is based on various global gender inequalities. ICRW funded the base line survey to establish benchmarks of various indices and understand the local context and value system that perpetuate violence against women and girls.
The study was carried out in 16 villages of a block in Surendranagar district, Gujarat. Listing of households was done to identify and list all girls aged 15-19 years, women aged 20-45 years and boys aged 18-22 years. The list was used for selecting 600 from each of the three groups - 400 each from intervention villages and 200 each from comparison villages. All selected respondents were interviewed using a pretested questionnaire. To maintain anonymity, few sensitive data pertaining to experience of sexual violence was self-administered by respondents with audio support on CAPI.
Response to each statement related to mobility, security, experience of harassment, and self-confidence and self-esteem were scored and by adding them for each parameter an aggregated score was developed. For each parameter, the aggregated scores were divided in three parts, low (<33%), middle (34-66) and high (>66). The aggregated scores indicates that more than 90% of girls and women gave medium score and rest gave a high score for believing that the places are secured. Similarly, majority girls (around 67%) believed in having right of accessing public spaces, and around 33% gave medium score. More women (60%) than girls (47-55%) scored medium on questions of experiencing any incidence of violence. Majority (65-74%) of women and girls scored high and around 30% medium with respect to levels of self-esteem and self-confidence. The difference between the respondents from experimental and comparison villages was mostly non-significant.

Malnourishment among children under 5 years continues to cause apprehension for all. Agro Tech Foods Ltd., an affiliate of Conagra Foods Inc. in partnership with Bharuch district administration provided peanut butter to children registered with Anganwadi Centres of three PHC areas over 9 months.
As monitoring and evaluation partner CORT assessed the impact of providing supplements on the growth of children on account of the intervention covering 69 AWCs in the intervention area, 25 in control area.
Experimental- control with pre and post survey design was used to assess impact of three different treatments in form of three different types of peanut butter provided to children. Longitudinal data in form of anthropometry measurements of children aged 24 -60 months registered with AWCs was collected at three points of time. Besides, AWW and mothers of children were also interviewed for their feedback on intervention.
Following intervention, normal category children for height for age indicator (stunted) increased by 15 percent point in intervention area while corresponding increase in control area was only 5 percent points. Difference in Difference (DID) of 9 percent point showing significant impact of peanut butter in intervention area. For weight for age Indicator (undernourished), percentage of children in the normal category increased from baseline to endline by 8 and 9 percent point in experimental and control area respectively showing no impact of intervention on undernutrition. Both AWW and mothers of children mentioned positive changes in children like weight of children has increased, more healthy and reported less sickness etc. following consumption of peanut butter.

Living Wage (LW) is defined as wage that should be adequate to allow workers to live a decent life and not in culture of poverty. Globally the concept of LW has been accepted by all stakeholders particularly Government, International agencies, employers. Many sustainability standard and certification organizations now include LW in their codes of practice.
The study funded by GIZ and Social Accountability International was undertaken to estimate LW of workers in garment industries located in Dhaka, its surrounding areas and satellite cities. Together they contribute 80% of the garment factories in Bangladesh. Differences in the cost of two areas, led to estimating two living wages.
Anker and Anker (2016) methodology was used to estimate LWs. All essential components of LW like diet, housing, health, education, and transportation were calculated separately by collecting a variety of data using mix methods of quantitative and qualitative approaches and triangulating all of this information to arrive at reasonable living wage estimates.
The estimated living wage for Dhaka, Bangladesh is Tk 16,245 ($211) and for satellite districts Tk13,314 ($173). These LW estimates that helps the worker to live decently are more than twice of prevailing wages. Large gap reflects very low wages received by garment workers compared to what is required to live decently but not extravagantly. In fact living wage uses conservative assumptions to estimate living costs for a basic but decent living standard. With current wages the garment workers bear a relatively high cost of housing with poor living standard.

Wages that a worker receives determines greatly their standard of living. Living Wage (LW) concept conceives that a worker should receive wages to sustain a decent life for his/her family but not being extravagant.
Tea is a labour intensive industry with export orientation. Nilgiri district produces 46 % of Tamil Nadu’s tea, with more than 50 % exported. In the present study, funded by Rainforest Alliance in partnership with ISEAL Alliance, LW is estimated for rural Nilgiris District, with focus on tea industry.
Anker and Anker methodology (2017) uses combination of secondary and primary data on basic elements of standard of living for a family which includes a low-cost nutritious diet, basic decent healthy housing, education of children, decent health care and other essential expenses. Information collected for each component was triangulated to estimate LW.
Monthly food costs for a family of four was estimated to be Rs. 8,113/-. While a decent house of 388 sq.ft. will cost around Rs.3,078/- towards rent, utility and opportunity cost. LW for tea workers is estimated to be Rs.11,422/- (June/ July 2018). This is 5% to 14% more than prevailing wages of workers on large tea estate, depending on size of year-end bonus given by tea estates. Quality of in kind benefits provided by tea estates falling within Plantation Act varies across estates. Living wage estimate are however higher (39% to 87%) than wages outside the tea sector for taxi drivers, restaurant workers and commercial shop workers.

Strengthening public health facilities with focus on quality improvement for maternal, neonatal and child health services is a step forward for tackling maternal and neonatal mortality, which continues to remain a high priority in health sector.
In 16 priority districts of Madhya Pradesh attempt was made to improve Quality Assurance measures by forming district quality team, capacity building and regular support /monitoring by team members of doctor. The intervention was made at all level of facilities: CHC - DH (L3 level), PHC- CHC (L2) l and SHC and PHC (L1).
The present study funded by MPTAST, FHI 360, was undertaken to assess quality of obstetric and newborn care services provided at L3 level (Comprehensive Emergency Obstetric and New born Care, CEmONC), L2 level (Basic Emergency Obstetric and New born Care, BEmONC) and L1 level of delivery points after the intervention.
A cross sectional survey using mix approach was used to collect data. In total 70 public health facilities across 16 districts covering 20 L1, 32 L2 and 18 L3 levels of services were studied. Besides service providers and IPD /OPD beneficiaries were interviewed.
Status of infrastructure, human resource, obstetric care, newborn care, pharmacy stock, infection control and bio waste management and IEC material were assessed for all the health facilities visited by the team. Using this data a composite index of quality of services was developed and percentage of total score achieved by the facility was calculated. Analysis revealed that majority ( 89 %) of L3 facilities fall in the ‘very good’ category (76% and above) , while L1 and L2 were in ‘good’ category (51-75%) with some exceptions. 97% of IPD and OPD beneficiaries were satisfied with services received in ward/facility. Medical officers faced constraints like shortage of staff, support staff, lack of equipment, non-functional equipment etc. in providing quality services.

With respect to most health indicators and utilization of health services for MCH care Bihar is significantly poor compared to national average. The Government of Bihar (GoB) with funding from DFID launched an integrated health, nutrition, water and sanitation programme called “Sector Wide Approach to Strengthening Health” (SWASTH).
For concurrent monitoring, CORT covered all 541 blocks in 38 districts of Bihar to collect information on selected health, nutrition, water and sanitation indicators. In all, 145,672 households, 79,229 women with children aged 0-5, pregnant and lactating women were interviewed. Besides, 22,657 different front line works of health/ICDS program, 9587 Panchayati Raj Institutions members and 267 block level officials including MO were interviewed. Besides functioning of 5,851 schools, 2,072 VHSND, 1,137 Bachpan divas and 100 THR sessions were also observed.
Block and district level analysis shows that a low proportion of women received ANC in first trimester (53%), or received 3 or more ANC check-ups (33%), 21% women consumed 100+ IFA tablets. Only 6% had full ANC consisting of three or more visits for ANC, received one TT injection and 100 IFA tablets/adequate amount of syrup consumed. Institutional delivery ranged from 36% in Sitamarhi to 77% in Rohtas and Jehanabad districts. Only 51% women received post-natal follow up within 48 hours or were visited by health worker within one week of delivery (48%). For children aged 6-24 months, 59% were exclusively breastfed till 6 months of age. The average months of exclusive breastfeeding were 5.5, the average age of introducing liquids was 6.6 months and semi-solid or solid foods were given by 7.7 months. Around 75% children 12-23 months had received full immunization.
Only 4 percent households treated drinking water to make it safer to drink. It was found that 16 percent households in Bihar had access to toilet facilities. Washing hands before eating meals was practiced by less than 6 percent and washing hands with soap after defecation was 36% ranging from 65% in Lakhisarai to 13% in Nawada.

Almost 56 percent of all under-five deaths in India are neonatal deaths. Testing interventions to improve neonatal survival that could be delivered in culturally acceptable way is a challenge. One such effort was taken by Micronutrient in the states of Uttar Pradesh and Gujarat.
The baseline survey undertaken in the two study states focused on measuring current levels of some of the key parameters which could be compared with the endline data to assess outcome of the intervention. Some of the key parameters included knowledge, attitude and practice of maternal, essential newborn, post-natal care and child health and nutrition.
The methodology used a cross sectional survey of a representative sample selected from the rural areas of two districts each of Uttar Pradesh and Gujarat. A total of 3,873 women who had delivered a child in last three years, were interviewed. Besides, qualitative data was collected by observing 121 health facilities and interviewing 268 providers consisting of 121 Medical Officers, 93 Nurses and 54 ANMs.
As expected, the results showed variations across the state and the two districts within the state. Majority mothers (77% in Basti and 90% in Dahod) delivered in health care facility but post natal visit within 48 hours of delivery was mostly neglected (25% in Maharajganj to 55% in Narmada). Mothers gave pre lacteal feeds (22-44% being least in Narmada), and delayed introduction to complementary feeding (6.3-6.9 months for liquids and 7.5-8.2 months for semi-solid food). Among children currently not breastfed, only 3-4% in Dahod and Basti and 12-19% children in Maharajganj and Narmada received minimum acceptable diet ensuring minimum dietary diversity and balanced mixture of different food groups. Such practices jeopardize the nutrition status of children.

The adolescent Life Skills Education (LSE) programme was an initiative implemented in Chandrapur district of Maharashtra. On a pilot basis it aimed to provide adolescents with a comprehensive set of life skills, making them aware of their rights, improving gender sensitization and personal development. The aim of the evaluation was to assess the relevance, efficiency, effectiveness and sustainability of the LSE initiatives and to analyse partner’s role in supporting the growth and development of the adolescents who were targeted by the initiatives. Using a combination of quantitative and qualitative techniques required data was collected. The quantitative data were collected through a survey of 1,200 students (600 boys and 600 girls) spread across 36 schools (ashram schools, Zilla Parishad/Nagar Parishad and private schools) in 15 blocks of Chandrapur district. Teachers, prerikas, peer educators and district /block level officers and partners were interviewed in-depth. Findings were analysed in accordance with the four criteria of relevance, effectiveness, efficiency and sustainability. Over 93% girls and boys reported that the programme helped them to develop in their everyday life. Positive accounts were also narrated by stakeholders (like teachers, block level officials) who felt that the project helped in addressing needs and priorities of school-going adolescent. Effectiveness of LSE programme was observed in behaviour changes and views of various stakeholders. LSE module facilitated the stakeholders to socialise and familiarise themselves with adolescents. Girls’ knowledge increased by 4.5 per cent more than that of boys as a result of the programme. Cost efficiency wise the programme cost per student was approximately Rs. 900/-. It will be a cost effective programme, if institutionalized. As LSE programme was a pilot initiative the implementing agency took it as an opportunity to test the feasibility of implementing the 24 programme sessions in local schools.

Child labour means employment of children (5 to 14 years of age) in gainful occupations, which are injurious to their physical, mental, moral and social development. Children working in hazardous occupations are more vulnerable to health hazards. ILO, New Delhi undertook the initiative of Convergence against child labour project: Support for India’s model to prevent and eliminate hazardous child labour. CORT undertook a survey of children in age group of 5 – 8 and 9-14 years working in hazardous sectors. The thrust of the study included identifying them, enrolment and absenteeism from school, understand causal factors that propel children to work and attitudes of working children, parents, employers and community towards child labour. The study spread over 10 districts of five states namely Bihar, Jharkhand, Odisha, Madhya Pradesh and Gujarat. A cross sectional sample survey was used to collect the required data using mix of quantitative and qualitative methods following listing. The target groups consisted of children (aged 5-14 years), parents of working children (5-14 yrs.), employers, and community members. The study listed 17698 working children and interviewed 3767 of these. Total coverage of parents interviewed was 1547, 258 employers and 403 community members. More than half of the working children reported to have migrated from rural areas. Main reasons for migration cited were ‘parents migration’ ‘poverty/ hunger’, ‘came to earn money’. With the main reason for children to start working being ‘poor financial condition’ and ‘family needed more income’. ‘More than half of working children were initiated into work at the age of 11-12 years. Almost all parents agreed that they played a role in employment of their children as ‘family needed more income’ and could not pay for ‘child’s education’. Majority of parents opined unhappiness about child’s involvement in work. Availability of amenities (school, health etc.) as explored from community members varied across the study areas.

Men who have sex with men (MSM) face high levels of stigma and discrimination in Indian society. It is a hard-to-reach (HTR) population at high risk for HIV. HIV prevalence among MSM is 4.4%, 13 times higher than general population, (0.35%).
FHI360 on an experimental basis dedicated 24 X 7 helpline using mobile technology in Chhattisgarh, Delhi and Maharashtra to reach MSM with messages and guidance to decrease their HIV risk behaviour and improve health-seeking practices.
Qualitative approach was used to assess the impact and reach of mSahaay in the study states. 41 in-depth interviews with MSM who had accessed mSahaay helpline, community mobilisers and 22 key informant interviews with service providers, government agencies and program implementing partners were conducted. A focus group discussion of helpline counselors was also organized.
MSM came to know about Sahaay largely through friends (peer educators), community mobilizers (bhaiya), Facebook, pamphlets and posters. Many of the friends and bhaiyas helped MSM in making their first call. Once the MSM were assured about confidentiality they then called 2-3 times. Most MSM found the helpline user-friendly, providing relevant counselling, and as they understood information provided. MSM and stakeholders appreciated mSahaay program and felt it has facilitated HTR MSM in providing a platform to share their concerns, problems and know about sources to seek treatment.
For sustainability and up scaling mSahaay, it is recommended for more publicity, linking with other services, use of multiple media like radio, TV. For scaling up, estimating number of locations where helplines lines are needed, number of counselors required, number of calls likely to be received, and peak timing remains a challenge. Continuous monitoring, training staff to provide information sought by MSM, adjusting program if required should be part of M&E activities.

Red Ribbon Express was world’s largest mass mobilization campaign that travelled 25,000 kms across 22 states implemented by National AIDS Control Organization (NACO), MOH and Government of India in the entire Nation. CORT with the funding from UNICEF monitored the program both at halt stations and outreach areas.
At each halt station, profile of visitors to the exhibition and other beneficiaries on boards were noted. A quick assessment survey was conducted covering 76 out of 152 (50%) stations between 2nd and 3rd week after the train had left the station. For each selected station, four spots where outreach activities were conducted were randomly drawn (304 spots), a listing of households was done to identify 40 households - 10 households each with presence of men and women aged 15-24 years and 25-49 years. The total sample covered in India was 12,159 households.
The average coverage of the people per station was around 25,000 ranging from 3864 in Uttarakhand to 71,740 Tamilnadu of whom 4% availed counselling, treatment for STI, testing for HIV and general health check-ups. The main activities done in the villages were role plays (62%), lectures (61%), announcements (44%), folk plays (35%), along with distribution of condom (20%), IEC materials. They were more knowledgeable about mode of transmission of AIDS, and 51% exposed against 31% not exposed to RRE knew at least three modes of transmission of infection by HIV. Exposed group (34%) had heard about sexually transmitted infections more than those not exposed (18%) to RRE.

Longitudinal Ageing Study in India (LASI) is focused on health, economic, and social well-being of India's elderly population. LASI is a national landmark in the scientific research, which facilitates an improved comprehension of India’s adult health problems and population aging processes and the design of appropriate evidence-based policies for adults and older people.
LASI focused on the socio- economic and demographic parameters of the household It include household economic status, health and biomarkers, health insurance and health care utilization, family and social network, work and employment, retirement and welfare programs for elderly. Biomarkers covered measurements and tests for blood pressure, pulse rate, height, weight, waist and hip measurements, timed walks, vision tests, grip strength, balance test, lung function test, cholesterol levels, and collection of dried blood spot (DBS) specimens.
CORT collected this baseline data from 80 primary sampling units covering three states including Jharkhand (2232 households), Odisha 2502 households and Maharashtra including Mumbai and Thane. A total of 129 PSUs were covered to cover 2512 households in Maharashtra. Data analysis and report writing will be done by the IIPS as nodal agency. The data and findings of the LASI wave 1 will be available for the researchers and policy makers shortly.
CORT proactively believes in enhancing utilization of the research findings. It has organized several national and international conferences on various themes, including, abortion, Gender Based Violence, youth, Millennium Development Goals, Child Labour, male involvement in RH, role of private practitioners in promoting different contraceptives, etc. Key program managers and stakeholders have attended these from both, national as well as international levels.
To ensure utilization of research findings, CORT uses variety of strategies and carefully identifies different segments of its audiences. To reach all segments of audiences, the information and research findings are packaged in different formats and disseminated through different channels including full report and power point presentation. In addition individual presentation as well as for specialized groups are also done. CORT had organized conference on Millennium Development Goals inviting stakeholders, program managers, researchers and implementers to discuss the challenges and way forward.



Capacity building is a mission of Centre for Operations Research and Training (CORT) in addition to evidence based research. CORT strongly believes in building technical skills of NGOs and other research institutions. Designing of the research project or social intervention, planning implementation, monitoring and mid-term correction, documentation of experience and techniques of effective communication to enhance utilization of research, its scaling up and scientific writing were addressed within the realm of maternal and child health and sexual and reproductive health. Realizing this CORT has made capacity building of researchers and NGO as one of its key mission and has tried to build capacity at all levels. In the process, CORT has developed vast experience and capability in capacity building both at individual level and organizational level training. To achieve this organizational objective, it organizes training workshops and provides internship to students, undertake research for demonstrating capacity building of officials at district level management and training of providers at different levels – doctors, community providers and front line workers.
Health policy of a nation contributes significantly in the country’s development by addressing health of the nation. Effective implementation of any health program at state and district level largely depends on the skills and capacity of the program managers in analysing the program statistics and Evidence Based Decision Making (EBDM).
The study was funded by Wellcome Trust along with Alliance for Health Systems and Policy Research at World Health Organization (WHO) and attempted to develop and test a model which ensures EBDM among program managers by institutionalizing capacity building. The project was implemented by a consortium of four partners consisting of CORT as prime, MOHFW Government of Gujarat (GoG), National Institute of Health and Family Welfare (NIHFW), New Delhi and International Institute for Population Sciences (IIPS), Mumbai.
In 6 districts of Gujarat, CORT along with GoG sensitized and build capacity of senior and middle level program manager, through a number of short trainings using an interactive hand holding approach, facilitating translation of learning’s to practice by individual interaction with program managers and group meetings in districts. Evaluation revealed significant increase in the EBDM capability of the program managers and some positive action. NIHFW, institutionalized EBDM training by including it as a part of training courses for program management unit personnel under NHM training. IIPS also institutionalized training by offering courses on EBDM and trained 150 students.
The multidisciplinary team of consortium partners had the scope to reach different target groups. Exposure to capacity building had motivated program managers to look into issues related to data and its utilization. Quality of data was perceived as felt need of program manager. It was also felt that some systematic changes are also essential to sustain effective utilization of the skills development of mid-level program managers. CORT trained programme managers at state, district and CHC/ Block/ PHC level in Gujarat with focus on issues related to data use for evidence based decision making at different levels of health sector.

CORT through short term training workshops tried to develop specific skills of the participants. Generally they were young and mid-level researchers working in different institutions. These were residential training workshops and the participants were mostly sponsored by their organization, Institutions like UNICEF, NACO, SIFPSA and some other funding agencies. In some cases the participants were self-sponsored. In the process CORT trained more than 270 participants from both within and outside the country. It included a range of participants like young social scientists, professionals, senior and mid-level program managers, doctors and paramedics as well as community health workers including peer educators. Research agencies and NGOs from neighboring countries that have benefited from the training courses include Bangladesh, Pakistan, Thailand, Nepal, Myanmar, Philippines, Indonesia and Malaysia. These were all in-person training workshops usually of around four days each. Training modality adopted are participatory in nature along with sharing of experience. Each training typically consisted of a formal teaching session followed by practical activities, like exercises, group discussions, classroom practicals and group presentations. Pre and post-test evaluation was normally done, which also provided a feedback to the organizers.
On the request of Care India, CORT organized special training in Delhi for their 25 Program Officers, Documentation and field based officers in operations research, monitoring and evaluation of their activities. CORT’s faculty members jointly visited institutions to give training to their officers. The training agenda was tailor made to meet their institutional requirement.
Topics covered in these training workshops are wide ranging which ultimately guided participants to objectively view their program, make strategic plans for effectiveness, continuously monitor their operations, etc. Substantive issues like Reproductive Tract Infection, Syndromic Approach, and Reproductive Health etc. has also been addressed. CORT also trained young social scientists in qualitative and quantitative data management and use of SPSS in data analysis in Social Science Research.

CORT has training as its one of the core competency. Knowing CORT’s strong commitment for capacity building, NACO, MoHFW, GoI entrusted responsibility of managing State Training and Resource Centre (STRC) in Gujarat, Ahmedabad and UT of Daman and Diu to CORT from 2008 to 2013. The focus of STRC was to provide training and build capacity of all 136 NGO partners who were implementing targeted intervention (TI) among high-risk groups for the AIDS Control Society of Gujarat, Ahmedabad and Daman & Diu. STRC aimed to ensure standardized and quality training to NGO staff implementing TIs by developing a sustainable and institutionalized centre for the capacity building of partner NGOs and community based organizations (CBOs) for TIs. It also aimed to gather learning through additional research and develop pedagogy of learning for TI scale up.
STRC trained TI partners to clearly visualize, plan and address their needs to saturate coverage of the high risk groups from getting HIV infection. It worked and trained the partner NGOs to ensure that the NACO guidelines for working with high risk populations in implementing TIs are properly followed and are put into action. It also recognized the importance of strengthening capacity of institutions to efficiently respond to the HIV/AIDS epidemic.
STRC worked with 136 NGOs to train around 13,500 TI staff by conducting more than 600 training sessions during 5 years on various themes and modules under TI guidelines of NACO. The trainees included 110 Project Directors, 490 Doctors, 210 Project Officers, 193 Counsellors and paramedics, 620 Outreach Workers, around 1200 Peer Educators and 130 community members. Besides, Monitoring and Evaluation Officers, Accountants of the TI partners and service providers including ANMs were also trained. The ORWs and PEs were trained and retrained to build their capacity in reducing the transmission of HIV during classroom training, and hand holding sessions during field training as well as exposure visits.
The themes covered included: Proposal writing, planning and management for implementing TI, basics of HIV/AIDS, condom promotion, harm reduction, Syndromic Case Management and basics of RTI/STI, human resource management, supportive supervision, induction training for new TIs, peer education, outreach planning, counselling skill, leadership, decision making, community mobilization and advocacy, developing learning site, crisis management, quality of care, referral, use of data, accounts and reporting, M&E, follow-up and documentation.
Besides, 215 master trainers and resource persons were raised covering each district. A dedicated webpage was assigned to STRC to give access to updated training calendar, training coverage, training reports and relevant modules, manuals and materials from other institutions.
Trainings were planned for 2 to 5 days following cascade model depending on the theme and type of participants. Trainings were organized at the district level in Gujarat and Daman where good training facilities were available to ensure participation of the doctors and other trainees and to reduce the cost of training and transportation. All the trainings were evaluated using pre and post-tests. Each year STRC-CORT conducted 120 trainings each with a batch of 25–35 trainees.
STRC-CORT secured grade A when NACO evaluated its work in July 2009 after three years of its functioning by an independent agency. After receiving a satisfactory and positive report of Evaluation Contract of STRC-CORT was extended for two more years. STRC was again evaluated in 2012 and graded as a good performing STRC. Thus, CORT managed STRC and build capacity of NGOs for five years from 2008 to 2012. Moreover, Gujarat State AIDS Control Society also felicitated the STRC- CORT twice during the State level World AIDS day celebrations for the activities.

Our multidisciplinary team members are there largely since beginning, performing with complete passion and dedication in striving towards organization goals.

Dr Khan is a globally recognized health consultant and OR expert and scaling up with keen interests in RCH, monitoring and evaluation, GBV, adolescent gender equity and capacity building. Earlier, he worked with Population Council for 25 years, retired as Sr. Program Associate and Regional Director for FRONTIERS program in ANE region. Before that he was GM with Operations Research Group for 15 years where he directed research and training activities. He has been member/chairperson of various national and international committees including HRP WHO, SVRI South Africa, MOH&FW, ICMR, IRR, NARI & NIN. He has published more than 100 papers & a dozen books on diverse topics.

She has PhD in Demography & M.Sc. in Anthropology. Experience of over 32 years in social science research, she integrates quantitative & qualitative research for policy relevant issues. Her expertise is in RCH and has worked intensively on issues like abortion, children, maternal health etc. Worked as PI/Co-PI for numerous projects supported by Govt., INGO & NGOs. Building capacity of social scientists is another area of work. She has contributed numerous papers in national/international journals.

She is PhD in Social Work and M.Sc. Dietetics and Organization Management. She has 32 years’ experience as PI/Co-PI in conducting large-scale quantitative and qualitative Social Science policy relevant research. For 5 years, she coordinated State Training and Resource Centre with NACO. As Program Officer, Population Council for 9 years she coordinated a Grants Program for strengthening RH research in Gujarat. She has contributed papers in national and international journals.

She has 29 years of experience in data processing of large scale quantitative surveys like NFHS, DLHS, facility survey and qualitative research. Develops data entry package for each study tools, with in-built range and consistency checks for data collection in CAPI. She also co-ordinates coding, office editing and data cleaning. She developed a MIS system for a project in MSU. Earlier, for 2 years she worked as Technical Assistant with ORG. She trains and provides technical assistance for data processing to university students and RAs.

She has 25 years of experience in social science research coordinating fieldwork in projects using quantitative and qualitative techniques. Her experience and expertise is in actual data collection for qualitative studies using FGDs, IDIs etc. eliciting responses to study issues. She also coordinates quantitative surveys. She trains, supervises and guides field teams. In qualitative data, she is involved in coding, analysis and triangulation of information. She has served as a trainer in CORT STRC activities.

He is with CORT for 12 years and has overall experience of 15 years for coordinating fieldwork. He has led field teams for number of surveys covering majority states of India. He trains, monitors and supervises field teams as well as actually collects data using techniques like FGD, IDIs, and key informant interviews from district and state level key stakeholders. He has coordinated large surveys like NFHS, RCH and facility surveys.

He is with CORT since 7 years and has experience of conducting fieldwork since 13 years with various other organizations. During his tenure with CORT, he has been involved in quantitative data collection. He has supervised teams for small and large scale surveys and travelled to major states. He coordinated teams in Longitudinal Ageing Study in India (LASI-Wave I, Phase II) in Jharkhand and NFHS-4 and NFHS-5 in Gujarat.

He is working with CORT since 1½ years. He has previously assisted a CA for B R Pancholi & Co., and worked as accountant with Rhythm Events & Promotions in Vadodara. He is skilled in account updates, financial statement review, corporate tax planning, Budget analysis, Account reconciliation and Tax accounting. He manages and reports data using Tally ERP 9 for project wise analyse. He calculates tax owed, prepares/submits returns and uphold compliance with applicable laws.
Thank you for your interest in CORT’s services.
Please provide the following information about your business needs to help us serve you better.